








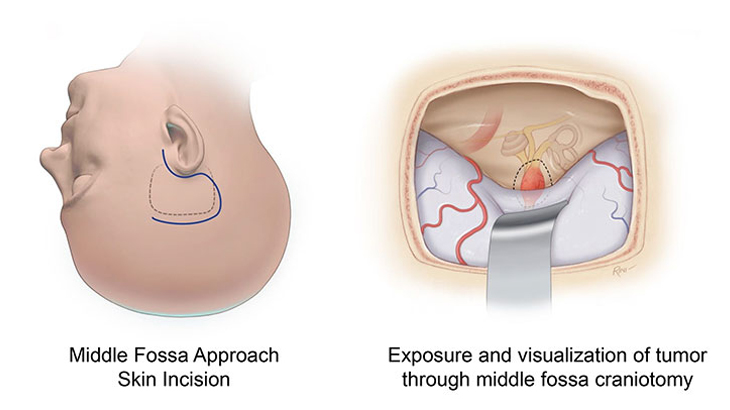
Middle fossa surgery
This approach is most commonly used for removal of smaller tumors when hearing is still intact. It is particularly useful for tumors under 1.5 cm and tumors located within the internal auditory canal next to the inner ear. It can also be utilized to decompress the bone around a tumor in the case of an only hearing ear allowing possible preservation of hearing for a longer period of time without requiring tumor removal and be utilized to help prevent facial paralysis in the case of a facial nerve tumor.
In addition to acoustic neuromas, this approach is also utilized to treat superior semicircular canal dehiscence, encephaloceles, and facial nerve decompression. In this approach, an incision is made above the ear and the brain is elevated to expose the tumor. Every effort is made to preserve hearing and still remove the tumor. In about 40% of cases, the tumor involves the hearing nerve or the artery leading to the inner ear and total loss of hearing results in the operated ear.
Advantages of the middle fossa approach
- Optimal for hearing preservation
- Versatile approach for many disorders including small acoustic neuromas
Disadvantages of the middle fossa approach
- Need for retraction of the dura and the temporal lobe
- Facial nerve is in a disadvantageous position
- Only useful for tumors smaller than 1.5 cm
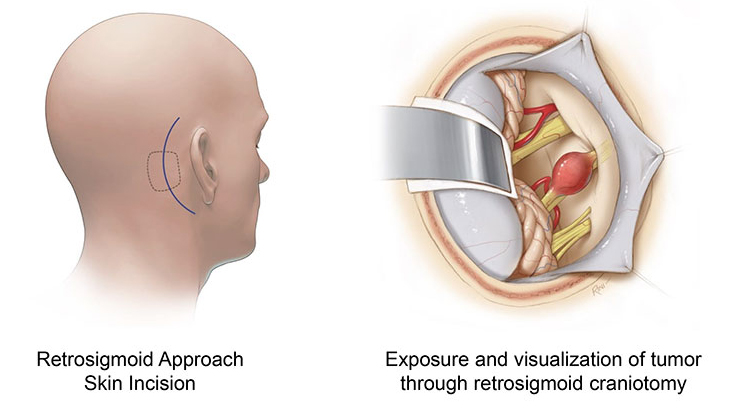
Retrosigmoid approach
This approach is utilized in cases where there is significant tumor extension towards the brainstem but less extension in the internal auditory canal towards the inner ear. In this approach an incision is made behind the ear and the brain is depressed to expose the tumor. In some cases, it is necessary to sacrifice the hearing to achieve tumor removal. In about 50% of cases, the tumor involves the hearing nerve or the artery leading to the inner ear and total loss of hearing results in the operated ear.
Advantages of the retrosigmoid approach
- Useful for tumors that extend towards the brainstem where hearing preservation may be desired
- Versatile approach that is useful for larger tumors in the cerebellopontine angle even when hearing preservation is not a factor
Disadvantages of the retrosigmoid approach
- May not be an optimal hearing preservation approach when the tumor extends close to the inner ear in the internal auditory canal
- May not be an optimal approach for patients with preexisting headaches
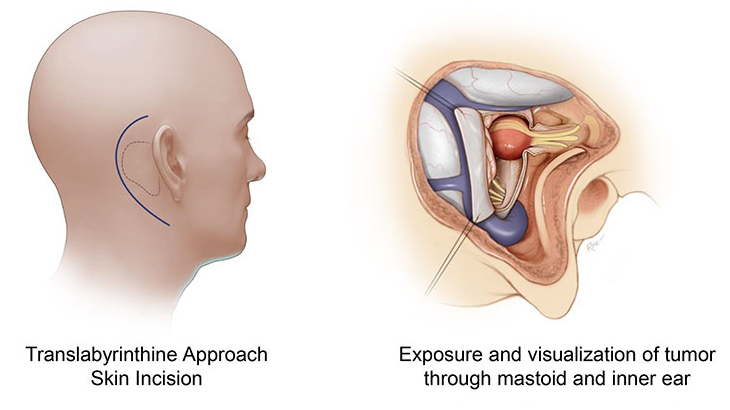
Translabyrinthine approach
This highly versatile approach can be utilized for any size tumor and is especially useful in large tumors where preservation of the facial nerve and its function are essential. This approach involves an incision behind the ear and allows one to identify the facial nerve before tumor removal and provides an access to the tumor by going through the mastoid bone and the inner ear. As a result, this approach is utilized for tumors where hearing preservation is unlikely. The mastoid defect is closed with fat taken from the abdomen. This approach results in a sacrifice of the hearing and balance mechanism of the inner ear. The balance mechanism in the opposite ear provides stabilization for the patient in one to four months.
Advantages of the translabyrinthine approach
- Versatile approach that allows safe removal of tumors of any size
- Upfront identification of the facial nerve and minimization of facial nerve complications
- Minimal retraction on the cerebellum
Disadvantages of the translabyrinthine approach
- Loss of hearing in the operated ear (permanent)
- Loss of balance function in the operated ear (permanent but compensated by opposite ear)
This approach is reserved for growing tumors and is not a hearing preservation approach. In the case of nongrowing tumors without significant symptoms, observation with serial imaging (MRI) is a reasonable option. The aim of SRT or Cyberknife for acoustic neuroma is to stop the tumor from growing further and while it can result in tumor shrinkage, it does not generally result in disappearance of the tumor. Treatment occurs in an outpatient fashion and is done in a team fashion with a radiation oncologist and a radiation physicist. Our job as neurotologists is to minimize the dose minimize dose to the cochlea and ensure that the radiation fields accurately encompass the tumor while minimizing effects of radiation beyond the tumor.
Advantages of the SRT for acoustic neuroma
- Outpatient, requires 5 days of treatment
- Minimal risk of facial nerve paralysis
- Generally recommended for growing tumors less than 2.5 cm
- Also, a reasonable approach for growing facial nerve tumors in patients with normal facial function.
Disadvantages of SRT for acoustic neuroma
- Small risk (1 in 1000 patients) of future malignant degeneration of tumor – risk can extend quite far out from treatment up to 10-15 years so serial monitoring with imaging is required.
- Generally, this approach is not hearing preserving. Hearing will likely decline over a longer period of time (5-10 yrs).
- Does not result in tumor removal so will require yearly monitoring.
Risks of all approaches
All of the following are risks of surgery for the above surgical treatments. We will discuss all of these risks as they relate to your clinical presentation.
- Facial paralysis
- Hearing loss
- Cerebrospinal fluid leak (through the ear or through the nose)
- Meningitis (infection of the lining of the brain stemming from an infection of the cerebrospinal fluid)
- Stroke
- Seizures
- Bleeding
- Infection
Our providers

Expert otolaryngology care
Getting the care you need starts with seeing one of our otolaryngologists.